PDHC — Planned Data in Healthcare — is a software platform built to support the coordination of patient care across organisations and providers in a Swedish healthcare context. A Vinnova-funded (2023–2028) public–private collaboration, the project demonstrates solutions that support the transition of healthcare from intervention-based care to continuous health management along the patient trajectory.
The central premise is straightforward: healthcare involves multiple parties — patients, clinicians, care providers, administrative staff — and the data that flows between them must be structured, secure, and standards-compliant. PDHC addresses this by decomposing the problem into discrete microservices that communicate through well-defined APIs, all grounded in the FHIR R5 specification, the most current version of the international standard for health data exchange.
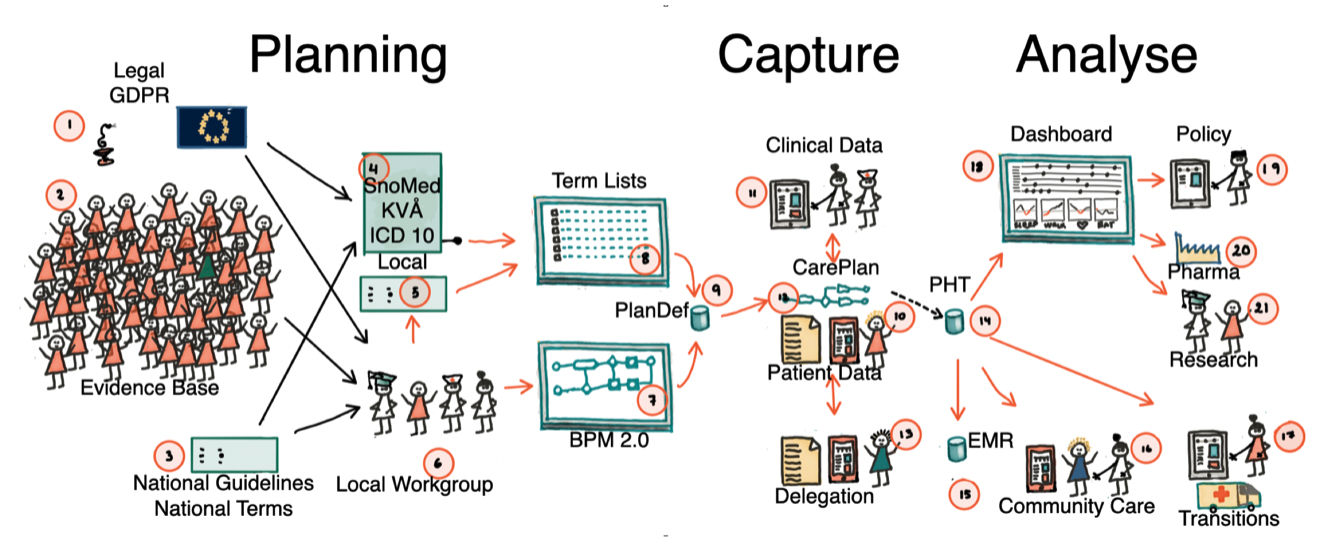
The project is based on preplanning data around locally developed healthcare processes. Once a workflow is defined, data collection can be fully structured and reused across EMRs, quality registries, and clinical research protocols. A better information service layer promotes interprofessional interoperability and patient participation.
Background
Semantic interoperability enables healthcare systems to share and understand data consistently, ensuring information keeps its meaning across settings. This is essential for outcomes-driven services, where accurate, comparable data is required to measure results, improve care quality, and drive evidence-based decisions. It is a foundation in the drive for personalised and precision medicine.
Subprojects
Subproject 1 — Specialty-Level Healthcare
Concomitant processes for collecting the correct information for better clinical management, EMR documentation, reporting to quality registries, and clinically embedded observational research. More than 800 patients have participated. Partners: Region Västra Götaland, Swedish Airway Quality Registry, Cambio, Karolinska Institutet.
Subproject 2 — Rare Diseases
Distributed support for patients with rare diseases. Standard information models for self-management support in rare diseases enable assistance for correct disease management across national borders. A forceful application of semantic interoperability standards simplifies real-time support and quality control. Partners: SOBI/FLORI, Karolinska Institutet.
Subproject 3 — Patient Self-Monitoring
Patient self-monitoring is highly desired by patients and providers. Current legislation and technical shortcomings have resulted in widespread development of monolithic solutions. While excellent within a single diagnosis and data stream, they become expensive and difficult to maintain. This subproject aims at understanding general requirements and real-world testing of interoperable solutions. Partners: Region Uppsala, Medituner AB, Cambio, Astma Allergi Förbundet.
Subproject 4 — Secondary Prevention in Heart Disease
Secondary prevention in heart disease could diminish further morbidity and improve quality of life. We have developed a simple administrative routine for calculating the need to meet the patient based on quality registry data, now aiming to connect this to secondary prevention support in primary health care. Partners: Region Uppsala, Karolinska Institutet, Novartis. Other partners will join.
Design Principles
Common to all activities are the following:
Local Planning Tools
Planning of care must be done with locally available tools
Real-time Feedback
Preplanning of data allows for real-time principles in feedback
Avoid Post-organisation
Avoid post-organisation of data due to costs and risk of errors
Standards First
Built on FHIR R5, with compatibility for OpenEHR, SNOMED CT, LOINC, and OMOP
Security by Design
OAuth 2.0 with PKCE, JWT tokens, audit trails, and rate limiting built into every service
Test Discipline
Every deployment step has corresponding tests — no step advances if its tests fail